Why Your 5 Whys Keep Blaming People: The Simple ‘System Why’ That Stops Fake Accountability At The Root
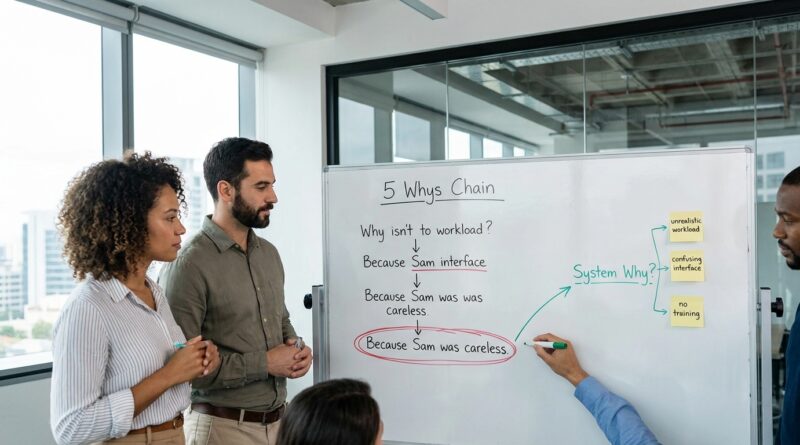
You know the meeting. Something goes wrong. A customer is upset, a deploy breaks production, a patient handoff gets messy, or a safety check is missed. The team runs a quick 5 Whys, and somehow the answer keeps landing on the same square. Someone should have been more careful. Someone should have followed the process. Someone should have spoken up. It feels like accountability, but it is mostly a neat way to stop thinking early. That is why the same problem keeps coming back with a different name and a different person attached to it. If your 5 whys root cause analysis blaming people vs system keeps ending with “human error,” you do not have a people problem first. You probably have a system question nobody asked. The fix is a tiny mental rule I call the System Why. Before you accept any people answer, ask one more question. What in the system made that action likely, easy, normal, or hard to avoid?
⚡ In a Hurry? Key Takeaways
- Your 5 Whys is probably off track if it ends with “they should have paid more attention” instead of a system condition that can be changed.
- Use one simple rule. After every human-action answer, ask, “What in the system made that likely or difficult to avoid?”
- This protects people and improves results, because blame rarely prevents repeat failures, but better design often does.
Why 5 Whys so often turns into blame
The 5 Whys is supposed to help teams get past the surface. In real life, it often does the opposite.
Why did the issue happen? Because Alex skipped a check.
Why did Alex skip it? Because he was rushing.
Why was he rushing? Because he did not manage time well.
And just like that, the trail ends with character judgment dressed up as analysis.
This happens because “human error” feels concrete. You can point to it. You can write it in a report. You can tell yourself the problem is handled because the person was reminded, retrained, or warned.
But if the same kind of failure happens again, with another decent employee under similar conditions, that is your clue. The person was the last stop in the chain, not the root of it.
The simple fix: add a “System Why”
Here is the rule.
Never let a human-action answer be the final answer
If a Why produces a statement about attention, effort, memory, judgment, or compliance, you are not done.
Ask one more question.
What in the system made this action likely, normal, tempting, or hard to avoid?
That is the System Why.
It is small enough to use in a five-minute review. It also changes the tone of the whole conversation. Instead of “Who messed up?” the room starts asking, “What setup made this outcome more likely?”
What counts as a system?
More than most people think.
A system can mean staffing, time pressure, tool design, unclear ownership, alert overload, bad defaults, training gaps, conflicting goals, missing checklists, confusing screens, weak handoffs, poor documentation, messy naming, hidden steps, or a process that only works on calm days.
In other words, the system is the environment people are operating inside.
A quick example
Let’s say a bad config change reaches production.
Blame version:
Why? The engineer entered the wrong value.
Why? They were not careful enough.
Action: remind engineers to pay more attention.
System Why version:
Why? The engineer entered the wrong value.
System Why: What made that likely or hard to catch?
Answer: Two fields had similar names, the review step was rushed because the on-call load was high, and the tool had no validation or preview.
Now you have things you can actually fix. Rename fields. Add validation. Reduce review pressure. Create a safer approval path for high-risk changes.
That is real accountability. Not softer. Better.
How to tell when your investigation is faking accountability
Watch for these phrases:
- “Should have paid more attention”
- “Failed to follow the process”
- “Made a poor decision”
- “Did not communicate”
- “Forgot”
- “Was complacent”
None of these are useless. But by themselves, they are incomplete.
People do forget. They do miss things. They do make bad calls. The point is not to pretend humans are perfect. The point is to ask why a normal imperfect human in that setting was able to create that outcome so easily.
If your report ends with a human trait and no design flaw, you probably stopped too soon.
The psychology behind this, in plain English
When something goes wrong, our brains zoom in on the person closest to the event. It is fast. It is emotionally satisfying. It gives us a story with a clear villain.
But systems are sneaky. They shape behavior quietly. Bad screens invite bad clicks. Overloaded teams skip “optional” steps. Confusing ownership leads to dropped handoffs. Metrics that reward speed over care push people toward risky shortcuts.
Once you see that, a lot of “employee problems” start looking like system problems wearing a human mask.
This is similar to a pattern outside the workplace too. If you have ever noticed that surface-level fixes rarely hold, the same logic shows up in Why Your Anxiety Fixes Never Stick: Use ‘Body-First Whys’ To Get Past Surface Triggers. Different topic, same lesson. If you stop at the visible reaction, you miss the conditions underneath that keep recreating it.
How to use the System Why in a five-minute 5 Whys
Step 1: Write the first human answer without shame
Do not ban human actions from the conversation. That backfires.
If someone skipped a step, write that down. If someone misread a field, say it plainly.
Then pause.
Step 2: Ask the System Why immediately
Use one of these prompts:
- What in the setup made that likely?
- What made the right action harder than it should be?
- What signal, tool, rule, or condition failed this person here?
- If three other good people were placed in the same situation, how many might do the same thing?
Step 3: Look for conditions, not character
Push the team toward facts you can change.
- Was the process clear?
- Was the interface confusing?
- Were expectations conflicting?
- Was there enough time, staffing, or support?
- Were there safeguards to catch the mistake before impact?
Step 4: Make at least one fix that does not depend on perfect human behavior
This is the big test.
If every action item is “retrain,” “remind,” or “tell people to be careful,” your analysis is weak. Those can help, but they should not be the whole plan.
Add a design fix. A checklist. A forced field validation. A second-person review on risky cases. Better labels. Fewer alerts. Clearer ownership. More realistic staffing.
What managers get wrong when they hear “don’t blame people”
Some hear this and worry it means lowering standards.
It does not.
You can still expect professionalism. You can still coach poor performance. You can still deal with reckless behavior when it is truly reckless.
But most recurring failures are not caused by one unusually bad person. They come from ordinary people working in messy conditions.
A good manager does not confuse punishment with prevention.
Three better questions than “Who dropped the ball?”
1. What made this make sense at the time?
This helps you understand the local reality. Maybe the shortcut saved ten minutes during constant interruptions. Maybe the warning looked like every other harmless warning.
2. What guardrail was missing?
Good systems assume human slips will happen and try to catch them early.
3. What would stop this if a tired, distracted, decent person did the same thing tomorrow?
That is the standard. Not ideal behavior on a whiteboard. Real behavior on a hard day.
When the answer really is partly about a person
Sometimes a person did ignore training. Sometimes they did cut corners knowingly. Fine. Say so.
Then still ask the System Why.
Why was one person able to bypass the safeguard so easily? Why did the process rely on private heroics or private honesty? Why was there no detection before damage happened?
Even when individual accountability is appropriate, system learning is still necessary.
At a Glance: Comparison
| Feature/Aspect | Details | Verdict |
|---|---|---|
| Blame-based 5 Whys | Stops at “carelessness,” “non-compliance,” or “poor judgment,” then assigns retraining or reminders. | Feels firm, but rarely prevents repeats. |
| System Why approach | Treats human action as a clue, then asks what conditions made it likely and what guardrails were missing. | Far more useful for real root cause analysis. |
| Action items produced | Can range from better tooling and workflow design to clearer ownership, staffing, and safer defaults. | Best option if you want fewer repeat incidents and less fear. |
Conclusion
If your 5 Whys keeps ending with “someone should have tried harder,” it is not giving you truth. It is giving you a shortcut. Across safety, healthcare, and tech, the message coming through loud and clear is that most “employee problems” are really system problems wearing a human mask. The useful shift is not complicated. Just add one micro-habit to every review. When the answer points at a person, ask what in the system made that behavior likely, normal, or hard to avoid. That one extra question can stop weaponized accountability before it hardens into culture. It can help stressed managers avoid lazy human error conclusions, protect good people from becoming the whole story, and fix the design flaws that keep creating the same failures quarter after quarter. Real accountability is not about finding the nearest person to blame. It is about changing the conditions so the problem is less likely to happen again.